")
Degenerative Disc Disease (DDD), Pinched Nerves and Proper Posture. How are they Related?
The Five System Approach to Treatment
*Mike is on sabbatical for the next several months – please call reception for details.
Through my 27 years of practicing massage therapy, I have had the opportunity to meet and treat many people with conditions, such as “Degenerative Disc Disease” (DDD).
 Patients, who receive this diagnosis from their physicians, often are left with the feeling of despair and hopelessness. Having said that, I wanted to write an article that can be useful to the reader in understanding DDD. Often, this condition is largely misunderstood or better yet, not understood. When a patient receives the diagnosis of DDD, this does not mean that he/she is disabled, and does not mean that they are headed for a downward spiral of health and further spinal degeneration. In fact, DDD tends to be part of the natural aging process that we all go through, to one extent or another. In this article, I hope to explain degenerative disc disease, the resulting signs and symptoms, and what can be done about managing this condition.
Patients, who receive this diagnosis from their physicians, often are left with the feeling of despair and hopelessness. Having said that, I wanted to write an article that can be useful to the reader in understanding DDD. Often, this condition is largely misunderstood or better yet, not understood. When a patient receives the diagnosis of DDD, this does not mean that he/she is disabled, and does not mean that they are headed for a downward spiral of health and further spinal degeneration. In fact, DDD tends to be part of the natural aging process that we all go through, to one extent or another. In this article, I hope to explain degenerative disc disease, the resulting signs and symptoms, and what can be done about managing this condition.
Firstly, we need to know a few facts about the body as it ages. Secondly, we need to have a general understanding of what the condition is, and thirdly, we need to know that what can be accomplished to mediate the effects of this condition. I will try to explain this in terms so that the general population can comprehend it, as many articles are written for the medical practitioner, and as so, not comprehensible to the general public.
What happens to our bodies as we age?
As we age, generally speaking, the body’s mobility starts to decrease. We start to feel somewhat stiff in the mornings, and it’s generally harder to get out of bed. The first 30 minutes in the morning are the worst and then the body starts to loosen or warm up. It also may be harder to find a comfortable position to lie in when going to bed. Turning over in bed might start to become a challenge, whereas before, you may have never given it a second thought. Yes, even sex might be difficult at times. I am sure this hits home with the reader who is now past forty five years of age. It is also common, for the younger population, not to relate to these signs of aging, as they have not yet experienced it.
These are all normal incremental symptoms people feel, usually starting at around 40 years of age. So why does this happen?
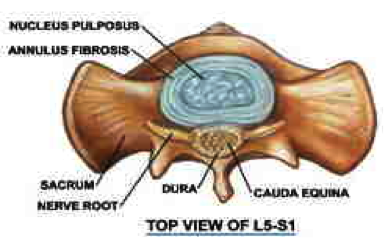
One of the many reasons, is when we are young, our intervertebral discs (IVD), which are situated or positioned between each vertebra in our spine, are full of a viscous fluid ( jelly-like material). This fluid is called the nucleus pulposus. The nucleus pulposus is in the center of each disc; whereas, the outside of the disc is a tough fibrous tissue called the annulus fibrosis. To give an analogy to this, discs are akin to a rubber tire on a car that is full of jelly, instead of air. The rubber tire is like the annulus fibrosis, and the air inside the tire is where the jelly like substance is.
I have heard it described as a jelly doughnut, but I do not think this is a good comparison, as a jelly doughnut would be far too weak to hold the jelly under the compressive loads of the spine.
As we age, the fluid in the disc becomes thicker and the annulus fibrosis degrades or weakens. The fluid becomes more like tar than jelly. Being a Canadian, I call this the “hockey puck syndrome”, as the disc become more like hockey pucks than tires full of jelly.
By the time we are 60 years of age, most of the fluid has transformed into this much thicker tar like fluid, than jelly. The outside of the disc, the annulus fibrosis, may become bulging and misshaped rather than a nice round tire. The tires now may have bulges in it.
This scenario primarily happens in the low back, between the fourth and fifth vertebrae and the fifth vertebrae and the sacrum. These are the L4 and L5 discs or IVDs.
Discogenic pain (pain arising from discs) can be felt in the low back when these discs are affected.
The cervical spine, or neck, is often affected as well, usually between C4-C5, C5-C6 and C6-C7. So the discs of C4,C5, and C6 can generate discogenic pain in the neck.
This degrading process of the discs is known as Degenerative Disc Disease or DDD.
In some people, as the discs degrade, the space for the nerves where they exit out of the spine, called the intervertebral foramina, or IVFs, becomes narrow. This narrowing, or stenosis, can put pressure on the nerves that exit the spine where they travel to the arms or legs.
When this narrowing/stenosis occurs in the neck, it can causes pressure on the cervical nerves. This is often called a “Pinched Nerve” which causes pain radiating or projected down the arm or leg. When pressure is applied to the nerves in the low back, or lumbar spine, it can cause a condition called Sciatica, which is when pain radiates down the back side of the leg to the heal. When the pressure is applied to the nerve roots at the neck, or cervical spine, the pain travels down the arm and sometimes into the hand depending on which nerve is compressed.
The most common area of compression in the neck is the C5 nerve root, this causes pain radiating over the shoulder/deltoid and outside of the upper arm or lateral brachial region. The most common area of compression in the low back is the L5 nerve root, which causes the pain radiating down the leg to the heel.
These areas of pain or sometimes numbness, are called the dermatomes, which are the areas of skin that are supplied by that particular nerve root. If the muscle is affected corresponding to the nerve root, this is called the myotome. Muscular weakness without any pain is possible when the myotome is affected and not the dermatome. If the dermatome is affected without the myotome, then pain or numbness is felt according to the nerve root being compressed. So, the symptoms are dependent on what is being compressed and where.
These conditions are known as peripheral nerve stenosis, which means a decrease in the opening for the nerves exiting the spine (IVF). These conditions can be very painful and limiting to functional activities such as walking, running, hiking and daily grooming activities, like brushing the hair and getting dressed. These activities can pose a real problem for some people who have this affliction.
Figure 1
www.nucleus+pulposus&tbm
Ok, now that we understand some of what may be happening with this condition (DDD), what can we do to mediate the conditions and it’s problematical affects?
Here is my “five system approach” to conservative treatment and management of DDD:
- Education
- Postural correction or mechanical extension of the spine
- Nerve mobilization and mechanical drainage
- Exercise therapy for core stability and cardiovascular health
- Therapist assisted maintenance for general spinal and musculoskeletal health
1. Education:
The client/patient must understand the condition and the musculoskeletal effects of poor posture including sitting and standing postures. A healthy spine is a spine that has gentle curves from front to back (anterior to posterior). The low back or lumbar spine should have a small curve forward called a lordosis. The middle back or thoracic curve should gently curve backwards, called a kyphosis. The neck or cervical spine should have a gentle curve forward, called a cervical lordosis. When these curves are increased or decreased, the result is an enormous amount of stress on the discs (IVD) and the facet joints in the spine.
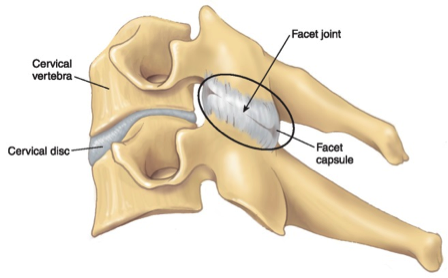
Let’s talk about the 3 joint complex for a moment.
The three joints that support each vertebrae, allow us to move freely and in multiple directions. They are the two facet joints on either side of the vertebrae (see figure #2 and the disc (IVD) in between each vertebrae). These three structures are known as the three joint complex. Each of these structures are designed to control and to attenuate specific loads onto the spine. When one of these structures is affected, the other two are also effected. One of these structures can’t be effected without the other being effected.
So when the disc is disrupted, so are the facets joints, and when the facets joints are disrupted so are the discs. This tri-complex is notably so connected that a mechanical disruption of any of the components of the “three joint complex” can lead to DDD and osteoarthritis of the spine. Compare this, if you will, to a car; if the tire is flat and you continue to drive on it, the wheel and bearings will break down. If the bearings and rim are not right, then the tire will break down. One of these 3 complexes can’t work without proper function of the other.
Results that are seen on imaging (MRI’s, x-rays, cat scans etc.) are that DDD and osteoarthritis of the facet joints go hand in hand with each other. The term that is used is Spondylosis.
Postural Correction. Again, and to reiterate, poor posture puts an enormous amount of pressure on the skeleton, especially the discs between the vertebrae. The truth is that gravity pulls us forward into a slumped posture. When you have a slumped or forward posture, there is a lot of pressure on the discs (IVDs), which causes discs to slowly degrade. Simple put, the fluid within the disc creates bulges in the annulus fibrosis and causes disc degeneration. This degeneration causes spinal, back pain and sometime leg and arm pain.
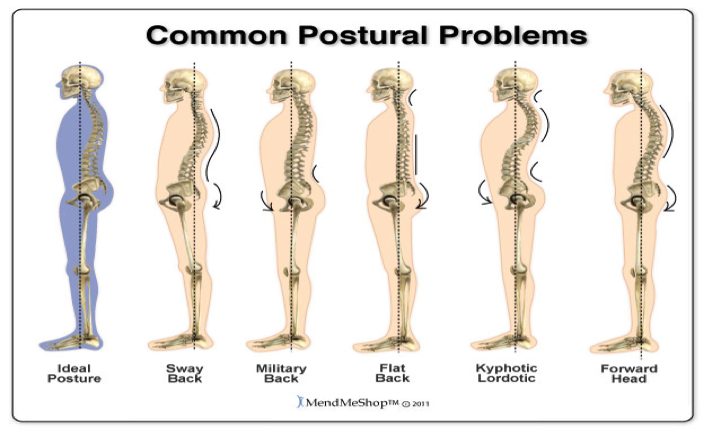
The following, is what I commonly see and observe every day in my practice. I will outline the following three dysfunctional postures:
a. Head forward carriage or posture.
b. Slumped posture with rounded shoulders (Hyperkyphosis).
c. Flattening of the low back (hypolordosis) and or exaggerated curve in low back (hyperlordosis)
a. Head forward carriage or head forward posture.
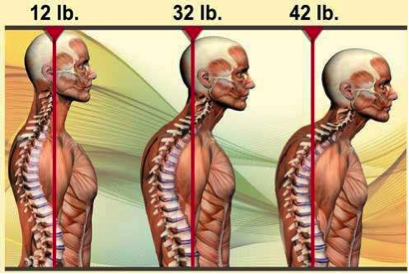
Most people have 1–3 inches of head forward carriage or posture. This is viewed and measured from the center of the ear to the center of the shoulder joint while looking at the side view of the person.
A rule of thumb, is that for every inch of head forward posture the neck (cervical spine) compression is equal to the weight of the head. So, for example, if the head weighs 8 pounds, and a head forward posture of 3 inches is noted, then this position adds an additional 24 pounds of stress on the discs (IVDs), and facet joints. This prolonged stress can lead to DDD. So, by correcting head forward carriage, it can unload the compressed discs and joints significantly. This procedure can reduce neck and arm pains and even reduce headaches. The solution is to do a mechanical correction of the head forward posture supported or followed up by specific exercise therapy.
Figure 3
http://ww w.google.ca
b. Hyperkyphosis or slumped forward posture of the upper thoracic spine and rib cage.
This is when the shoulders are rounded forward, and the spine is rounding too far backwards. The muscles in the back are too weak and the chest muscles are too short and tight. The back muscles have what is known as stretch weakness.
The rib cage starts to compress in the front of the body. This posture generates pain in between the shoulder blades, upper back tension, and stress in the trapezius and related muscles. Myofascial pain can result from the weakened back muscles which are over stretched. Some of these muscles develop active trigger points which can generate severe muscle-skeletal pain.
In this typical posture, the muscles in the back are constantly contracting to try, unsuccessfully, to right or correct the person’s posture (fighting against gravity).
This muscle-skeletal condition is an extremely common complaint of slumped posture or hyperkyphosis. Along with muscle-skeletal pain, the cardiovascular (heart-lung) system is compromised as the heart and lungs get compressed between the spine and the rib cage/sternum (chest bone). The abdominal organs can also be negatively affected due to compression and lack of proper nerve flow from the spine to the organs and visceral tissue. For example, with the condition of hyperkyphosis, I have found a correlation to a condition called Gastroespogeal Reflux Disease or GERD (see Published article in Massage Therapy Canada Magazine, Fall 2011)
It is my experience that long standing cases of GERD have had remarkable positive changes, with reduction of the symptoms of this disease, after performing a mechanical reduction of the hyperkyphosis. Muscle-skeletal pain often resolves with this correction and specific exercise therapy.
Figure 4-3A is hyperkyphosis and 3b is normal
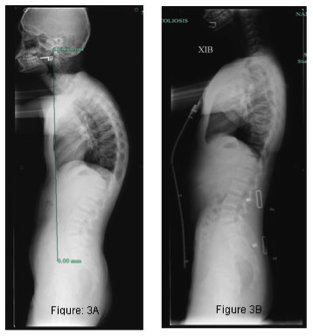

Figure 4. http://www.posturetek.com
c. Flattening of the low back (hypolordosis) and or exaggerated curve in low back (hyperlordosis)
This is when the lower back flattens out and the gluteals (bum muscles) start to shrink or flatten (muscular atrophy). This flattening is most notably found in the aging population, with males being affected more than females. This posture puts undue stress on the discs (IVF) in the low back (Lumbar spine).
To understand the mechanics of this, normally the discs support about 75% of the weight of the trunk, and the corresponding facet joints about 25% of the weight of the trunk. When this ratio is disrupted or changed, the degenerative changes can occur. With a flat back posture, the discs (IVDs) attenuate or support 100% of the load. This added stress compresses the discs into flat arrangement creating possible herniations or disc derangements (bulging tires). This derangement can lead to DDD. A wrong lift or twist can spell disaster with the herniation of a disc resulting is sever spinal pain and likely sciatica.
Hyperlordosis or an exaggerated lumbar curve
On the other hand, if the low back curve is exaggerated, then the facet joints are over compressed, which can lead to degeneration of the facet joints. The condition where the facet joints degenerate is called degenerative joint disease or DJD or Spondylosis. These two conditions often occur simultaneously. Severe back pain can be the result of either of these two conditions, or the two conditions coexisting.
Fiqure 5
So, I come back to what can be done about treating spinal pain and conditions associated with it, like degenerative disc disease, and degenerative joint disease. I have clinically found that mechanically correcting the posture and to reshape the intervertebral disc goes a long way to reducing or eliminating back and nerve pain. Especially conditions like Sciatica and radiating limb pain caused from peripheral stenosis (pressure on the nerve roots). How is this procedure performed, and what are the effects of this procedure?
2. Postural extension or mechanical extension of the spine:
The process is quite passive and done only to the patients comfort levels. The patient will lie face down on a specially designed treatment table, after receiving massage to the back muscles to soften the muscle tissue and reduce tension. The patient is covered with a blanket or towel. A broad strap is placed over the low back or mid back (the area to be treated). Slowly, the patient is extended (bent backwards) with the use of the moving parts of the table. This is done only to the patient’s comfort level. Traction is then applied to the spine to decompress the facet joints.
The position of extension allows the viscous fluid within the discs to shift towards the front side of the disc (anteriorly) shifting away from the back side of the disc. The shifting of the fluid take the pressure off of the backward side of disc (posterior wall) ligaments and supporting structures allowing the body to regain the proper spinal curves and alignment.
See below the pictures of the before and after the passive extension treatment
Before passive extension treatment

After passive extension treatment

Passive extension to the lumbar spine

3. Nerve mobilization and mechanical drainage of nerves:
Pain that travels down a limb, whether it is an arm or a leg, usually means the nerve associated with that body part is likely being compressed at the nerve root level. The nerve root compression can lead to radiating pain, loss of motor control (muscular weakness) and or loss of autonomic function (blood vessel control) which affects the blood flow, which in turn can cause swelling in the limb. People that suffer from Sciatica or a pinched nerve in the neck can well relate to these symptoms.
Nerve mobilization and mechanical drainage of the nerves helps to decrease the swelling within the nerve to allow for better functioning of the neurovascular bundles. These techniques help to restore proper functioning to the nerves and therefore the quicker return to normal functional activities of daily living. These techniques are not within the scope of this article but have been well described by the works of Dr. David Decamillis and Dr. David S. Butler.
4. Exercise therapy for core stability and cardiovascular health:
To support the postural corrections, proper strengthening and stretching exercises are indicated, as spinal alignment needs proper strength-length balance of supporting muscular tissue. Core stability exercises have been well documented to help the body recover from spinal conditions and muscular skeletal injuries. These type of exercises should be incorporated into an exercise program to maintain proper health and function of our bodies.
Cardiovascular health benefits should not go without mention, as a strong cardiovascular system has a plethora of positive benefits for the human body including muscular-skeletal and systemic health.
The above three elements: stretching and strengthening, core stability exercises and cardiovascular training are needed for proper alignment, musculoskeletal health, and overall healthy body conditioning.
5. Therapist assisted maintenance for general spinal and musculoskeletal health:
In today’s living and world, due to the ergonomics of the workplace, i.e. sitting and working on the computer and many other factors of activities of daily living, everyone needs some help, guidance and reminders for health. This should include mechanical correction of posture for the majority of the population. I call this the “spinal tune up”. Many of my patients will book appointments for the spinal tune up which includes the postural correction techniques and exercise recommendations. Patients will often say something like: “Wow I feel straighter”, or, “My body feels like it is taller”. One athlete reported feeling like she had an extra lung. One patient reported that his GURD had completely gone away after having it for 19 years.
Regular spinal maintenance is much better than treating acute injuries, such as a herniated disc or unrelenting back pain. I recommend monthly or even bimonthly corrective extension procedures to maintain spinal health and proper posture.
Summary
In this article I have tried to give the reader an understanding of how conditions like degenerative disc disease, back pain, and faulty posture are treatable conditions with positive outcomes. I would hope that the reader will gain some insight into maintaining spinal health and will seek out regular therapy for these conditions. This could mean seeing registered massage therapists, chiropractors or physiotherapists, to mention a few professionals, which can help.
I, being a registered massage therapist for over 20 years, have had extensive training in this field and have had the opportunity to train many new massage therapists with respect to treating the conditions above.
If you are having back pain, or if you have been given the diagnosis of degenerative disc or joint disease, there is help.
Contact the Electra Health Floor and increase your ability to perform your activities of daily living that you enjoy and deserve!
Mike Dixon RMT
www.electrahealthfloor.com
www.arthrokinetic.com
Definitions and Descriptions
- “Degenerative Disc Disease”. “One or more intervertebral disc(s) of the spine, often called “degenerative disc disease” (DDD) or “degenerative disc disorder,” is a condition that can be painful and can greatly affect the quality of one’s life. Disc degeneration is a disease of aging, and though for most people is not a problem, in certain individuals a degenerated disc can cause severe chronic pain if left untreated
http://en.wikipedia.org/wiki/Degenerative_disc_disease - The annulus fibrosis is the tough circular exterior of the intervertebral disc that surrounds the soft inner core, the nucleus pulposus. This outer portion is composed of a ring of ligament fibers that encases the inner core of the disc and securely connects the spinal vertebrae above and below the disc
Annulus Fibrosis Definition – Spine-Health
www.spine-health.com/glossary/annulus-fibrosus - Nucleus pulposus is the inner core of the vertebral disc. The core is composed of a jelly-like material that consists of mainly water, as well as a loose network of collagen fibers. The elastic inner structure allows the vertebral disc to withstand forces of compression and torsion. www.spine-health.com/glossary/nucleus-pulposus
- The Intervertebral foramina is between every pair of vertebrae are two apertures (openings), the intervertebral foramina (singular: foramen; also called neural foramina and often abbreviated as IV foramina or IVF). http://en.wikipedia.org/wiki/Intervertebral_foramina
- Stenosis is a reduction in the space available for nerve roots to exit the spinal canal is the definition of foraminal narrowing. Pairs of nerve roots branch off the spinal cord at every vertebral level through openings called intervertebral foramina (singular: foramen).
Foraminal Narrowing Definition – Laser Spine Institute
www.laserspineinstitute.com/back_problems/foraminal_narrowing/def/ - Spondylosis is a term referring to degenerative osteoarthritis of the joints between the center of the spinal vertebrae and/or neural foramina. If this condition occurs in the zygoapophyseal joints, it can be considered facet syndrome. If severe, it may cause pressure on nerve roots with subsequent sensory and/or motor disturbances, such as pain, paresthesia, or muscle weakness in the limbs.
http://en.wikipedia.org/wiki/Spondylosis - A myotome is the group of muscles that a single spinal nerve root innervates.[1]Similarly a dermatome is an area of skin that a single nerve innervates. In vertebrate embryonic, a myotome is the part of a somite that develops into the muscles.
http://en.wikipedia.org/wiki/Myotome - A dermatome is an area of skin that is mainly supplied by a single spinal nerve.[1]There are 8 cervical nerves (C1 being an exception with no dermatome), 12 thoracic nerves, 5 lumbar nerves and 5 sacral nerves. Each of these nerves relays sensation (including pain) from a particular region of skin to the brain.
http://en.wikipedia.org/wiki/Dermatome_(anatomy) - Degeneration of one or more intervertebral disc(s) of the spine, often called “degenerative disc disease” (DDD) or “degenerative disc disorder,” is a condition that can be painful and can greatly affect the quality of one’s life. Disc degeneration is a disease of aging, and though for most people is not a problem, in certain individuals a degenerated disc can cause severe chronic pain if left untreated.
http://en.wikipedia.org/wiki/Degenerative_disc_disease
References
- http://www.laserspineinstitute.com/back_problems/spinal_anatomy/lumbar_pain/
- Joint Play the Right Way for the Axial Skeleton 3rd edition 2006, Arthrokinetic Publishing
- http://www.arthrokinetic.com
- http://en.wikipedia.org/wiki/Degenerative_disc_disease
- www.spine-health.com
- www.laserspineinstitute.com/back_problems/foraminal_narrowing/def/
- http://drdavedecamillis.com/
- http://drdavedecamillis.com/articles/scans/MechanicalDrain_DeCamillis.pdf
- http://drdavedecamillis.com/articles/pubmed/DifferentiallyDiagnosingMechanicalLowBackPain_DDeCamillis.pdf
- http://en.wikipedia.org/wiki/Spondylosis
- www.spine-health.com/glossary/annulus-fibrosus
- http://prohealthsys.com/
- Orthopedic Physical Assessment, 4th edition, David J. Magee 2002
- http://www.massagetherapycanada.com/
- http://en.wikipedia.org/wiki/Myotome
- http://en.wikipedia.org/wiki/Dermatome_(anatomy)
- http://en.wikipedia.org/wiki/Degenerative_disc_disease
- www.noigroup.com/en/product/nsbe
- Carolyn Kisner, M.S., PT, & Lynn Allen Colby, M.S., P.T.: Therapeutic Exercise, Fourth Edition, 2002
- Cynthia C. Norkin, EdD, PT & D. Joyce White, DSc, P.T.: Measurement of Joint Motion A Guide to Goniometry, Third Edition, 2003
- Darlene Hertling, B.S., R.P.T., Randolph M. Kessler, M.D.: Management of Common Musculoskeletal
- Disorders, Physical Therapy, Principles and Methods, Second and Third Editions, 1996
- David J. Magee, PhD., B.P.T.: Orthopedic Physical Assessment, Second and Third Editions, 1996
- Philip E. Greenman, Priniciples of Manual Medicinge, second edition
- Frank H. Netter, M.D., Atlas of Human Anatomy 1993, The CIBA Collection of Medical Illustrations, 1991
- Janet G. Travell, M..D., David G. Simons, M.D.: Myofascial Pain and Dysfunction, The Trigger Point Manual, Volume 1 & 2, 1992
- Joseph E. Muscolino, The Muscular System Manual- The Skeletal Muscles of the Human Body, 2005
- Joseph E. Muscolino, Kinesiology: The Skeletal System and Muscle Function
- Laura K. Smith, Elizabeth L. Weiss, L. Don Lehmkuh. : Brunnstrom’s Clinical Kinesiologly. 5th edition
- Nikita A. Vizniak, D.C. Clinical Consultant Physical Assessment, Second Edition, 2005.
- Pamela K. Levangie, Cynthis C. Norkin: Joint Structure and Function a comprehensive analysis, third edition
- Robert B. Salter, MD, Textbook of disorders and injuries of the musculoskeletal System
- Robert E. McAtee, Facilitated Stretching 1993
- Stanley Hoppenfeld, M.D.: Physical Examination of the Spine & Extremities, 1976
- Steve Anderson, RMT, BSc.: Anatomy and Kinesiology lecture notes, 1992
- Susan L. Edmond, M.P.H., P.T.: Manipulation Mobilization and Spinal Techniques, 1993
- Taber’s Cyclopedic Medical Dictionary, 1983
- Carolyn Kisner, Lynn Allen Colby: Therapeutic Exercise Foundations and Technique